

 English
English Bahasa Melayu
Bahasa Melayu Bahasa Indonesia
Bahasa Indonesia Tiếng Việt
Tiếng Việt ไทย
ไทย
本翻譯僅作學術交流用,無商業意圖,請勿轉載,如有疑議問請來信
巴西聖保羅大學最新研究顯示,三酸甘油酯與高密度脂蛋白膽固醇(TG/HDL-c)比值異常,可能是動脈粥樣硬化脂質概況的重要指標。該比值的升高與冠心病的發展風險密切相關。研究分析了374名高風險患者,發現TG/HDL-c比值是預測冠心病程度的最強獨立指標。
三酸甘油酯與高密度脂蛋白膽固醇的高比值預測廣泛性冠心病。
High Ratio of Triglycerides to HDL-Cholesterol Predicts Extensive Coronary Disease
Protasio Lemos da Luz,I Desiderio Favarato,I Jose Rocha Faria-Neto Junior,II Pedro Lemos,I and Antonio Carlos Palandri ChagasI
IInsituto do Coração, Faculdade de Medicina da Universidade de São Paulo – São Paulo/SP, Brazil
IIFaculdade de Medicina, Pontifícia Universidade Católica do Paraná – Paraná, Brazil
Email: rb.psu.rocni@pzulad
Clinics. 2008 Aug; 63(4): 427–432.
doi: 10.1590/S1807-59322008000400003
PMCID: PMC2664115
PMID: 18719750
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2664115/
Abstract
An abnormal ratio of triglycerides to HDL-cholesterol (TG/HDL-c) indicates an atherogenic lipid profile and a risk for the development of coronary disease.
OBJECTIVE
To investigate the association between lipid levels, specifically TG/HDL-c, and the extent of coronary disease.
METHODS
High-risk patients (n = 374) submitted for coronary angiography had their lipid variables measured and coronary disease extent scored by the Friesinger index.
RESULTS
The subjects consisted of 220 males and 154 females, age 57.2 ± 11.1 years, with total cholesterol of 210± 50.3 mg/dL, triglycerides of 173.8 ± 169.8 mg/dL, HDL-cholesterol (HDL-c) of 40.1 ± 12.8 mg/dL, LDL-cholesterol (LDL-c) of 137.3 ± 46.2 mg/dL, TG/HDL-c of 5.1 ± 5.3, and a Friesinger index of 6.6 ± 4.7. The relationship between the extent of coronary disease (dichotomized by a Friesenger index of 5 and lipid levels (normal vs. abnormal) was statistically significant for the following: triglycerides, odds ratio of 2.02 (1.31–3.1; p = 0.0018); HDL-c, odds ratio of 2.21 (1.42–3.43; p = 0.0005); and TG/HDL-c, odds ratio of 2.01(1.30–3.09; p = 0.0018). However, the relationship was not significant between extent of coronary disease and total cholesterol [1.25 (0.82–1.91; p = 0.33)] or LDL-c [1.47 (0.96–2.25; p = 0.0842)]. The chi-square for lineartrends for Friesinger > 4 and lipid quartiles was statistically significant for triglycerides (p = 0.0017), HDL-c (p = 0.0001), and TG/HDL-c (p = 0.0018), but not for total cholesterol (p = 0.393) or LDL-c (p = 0.0568). The multivariate analysis by logistic regression OR gave 1.3 ± 0.79 (p = .0001) for TG/HDL-c, 0.779 ± 0.074 (p = .0001) for HDL-c, and 1.234 ± 0.097 (p = 0.03) for LDL. Analysis of receiver operating characteristic curves showed that only TG/HDL-c and HDL-c were useful for detecting extensive coronary disease, with the former more strongly associated with disease.
CONCLUSIONS
Although some lipid variables were associated with the extent of coronary disease, the ratio of triglycerides to HDL-cholesterol showed the strongest association with extent.
Keywords: Lipids, Triglycerides, HDL, Cholesterol, Coronary disease
摘要
三酸甘油酯與高密度脂蛋白膽固醇(TG/HDL-c)異常比值表示一種動脈粥樣硬化脂質概況,並預示著冠心病的發展風險。
目的
探討脂質水平,特別是TG/HDL-c,與冠心病的程度之間的關聯。
方法
高風險患者(n = 374)接受冠狀動脈造影檢查,測量其脂質變數,並使用弗里辛格指數評分冠心病程度。
結果
受試者包括220名男性和154名女性,年齡57.2 ± 11.1歲,總膽固醇210± 50.3 mg/dL,三酸甘油酯173.8 ± 169.8 mg/dL,高密度脂蛋白膽固醇(HDL-c)40.1 ± 12.8 mg/dL,低密度脂蛋白膽固醇(LDL-c)137.3 ± 46.2 mg/dL,TG/HDL-c 5.1 ± 5.3,和弗里辛格指數6.6 ± 4.7。冠心病程度(以弗里辛格指數5分為界)與脂質水平(正常 vs. 異常)之間的關係在統計學上顯著,對以下指標來說更為明顯:三酸甘油酯,勝算比2.02(1.31–3.1;p = 0.0018);HDL-c,勝算比2.21(1.42–3.43;p = 0.0005);以及TG/HDL-c,勝算比2.01(1.30–3.09;p = 0.0018)。然而,冠心病程度與總膽固醇 [1.25(0.82–1.91;p = 0.33)] 或LDL-c [1.47(0.96–2.25;p = 0.0842)] 之間的關係不顯著。用於弗里辛格指數 > 4 和脂質四分位數的線性趨勢的卡方檢驗結果,在三酸甘油酯(p = 0.0017)、HDL-c(p = 0.0001)和TG/HDL-c(p = 0.0018)方面在統計學上顯著,但對於總膽固醇(p = 0.393)或LDL-c(p = 0.0568)則不明顯。多變量分析的邏輯回歸OR值為1.3 ± 0.79(p = 0.0001)的TG/HDL-c,0.779 ± 0.074(p = 0.0001)的HDL-c,以及1.234 ± 0.097(p = 0.03)的LDL-c。接受特徵操作特徵曲線分析表明,僅TG/HDL-c和HDL-c對於檢測冠心病的程度有用,前者與疾病的關聯更為強烈。
結論
儘管某些脂質變數與冠心病程度相關,但三酸甘油酯與高密度脂蛋白膽固醇之比值與程度之間的關聯最為顯著。
關鍵詞:脂質、三酸甘油酯、HDL、膽固醇、冠心病
引言
脂質異常長期以來一直被懷疑對於動脈粥樣硬化有貢獻;幾項流行病學和世代研究已經確立了總膽固醇、低密度脂蛋白膽固醇(LDL-c)或低高密度脂蛋白膽固醇(HDL-c)與動脈粥樣硬化相關疾病(如缺血性心臟病、中風和周邊血管疾病)發病率之間的強烈聯繫。
最近,脂質粒子亞分別也被認為參與動脈粥樣硬化過程。小而密度高的LDL粒子比大而浮力較大的粒子更容易引起動脈粥樣硬化,而不同的HDL亞分別在動脈粥樣硬化過程中扮演不同的角色。較大且密度較低的HDL2粒子被認為具有保護作用,而小而密度高的HDL3粒子具有動脈粥樣硬化作用。前者與血清三酸甘油酯和小而密度高的LDL呈反向相關。三酸甘油酯與高密度脂蛋白膽固醇比值(TG/HDL-c)與血漿中小而密度高的LDL粒子水平呈反向相關。TG/HDL-c比值為3.8將LDL表型的分佈劃分為兩類,其中79%的B型表型大於此值,而81%的A型表型低於此值。我們最近分析了血漿脂質與冠狀動脈疾病(CAD)的發展之間的關係,表現為心絞痛、陽性缺血測試或冠狀動脈造影中存在重要的阻塞性病變。我們發現,TG/HDL-c比值 > 4 是CAD發展的最有力獨立預測因子。因此,這個比值顯示了它有望作為血漿脂質概況的動脈粥樣硬化指標的有吸引力替代品。然而,目前關於TG/HDL-c比值與冠心病病變的程度或嚴重程度之間的關聯的數據有限。
研究目標
評估脂質變數,特別是TG/HDL-c比值,與接受懷疑冠心病檢查的患者的冠狀動脈病變程度之間的相關性。
研究設計
符合資格的患者是門診患者,他們接受了懷疑冠心病的診斷性冠狀動脈造影。
危險因素的存在定義如下:高膽固醇血症(總膽固醇 > 200 mg/dL)、高三酸甘油酯血症(> 150 mg/dL)、高低密度脂蛋白膽固醇(LDL-c)(> 130 mg/dL)、低高密度脂蛋白膽固醇(HDL-c)(男性 < 40 mg/dL,女性 < 50 mg/dL)、升高的TG/HDL-c比值(> 4)、糖尿病(空腹血糖 ≥ 126 mg/dL,偶然或口服降血糖藥物或胰島素的GTI超過200 mg/dL或當前吸煙者的使用),高血壓(收縮壓/舒張壓分別為140/90 mm Hg),以及當前吸煙者。
使用標準技術進行總膽固醇和膽固醇分數、三酸甘油酯和血糖的實驗室測試。
使用Friesinger指數評估冠狀病變程度。該分類包括以下類別:0,無動脈造影異常;1,輕微異常(病變範圍為1-29%);2,病變範圍為30-68%;3,同一血管中多處狹窄,且該段具有一個或兩個病變,病變形態定義為多處、分散或管狀,或者兩個段落的狹窄為30-68%;4,至少一個病變為69-100%,除了近段應低於100%;以及5,一個血管近段的閉塞。左主病變被計為左降支和迴旋支的近段病變。冠狀病變由對患者脂質概況不知情的專家評分。
統計學
統計學分析使用卡方檢驗和非參數性ANOVA(Kruskal-Wallis)進行單變量分析,然後使用逐步向前的邏輯回歸進行多變量分析,以評估脂質變數對冠狀病變程度的獨立影響,分為Friesinger指數5。
研究結果
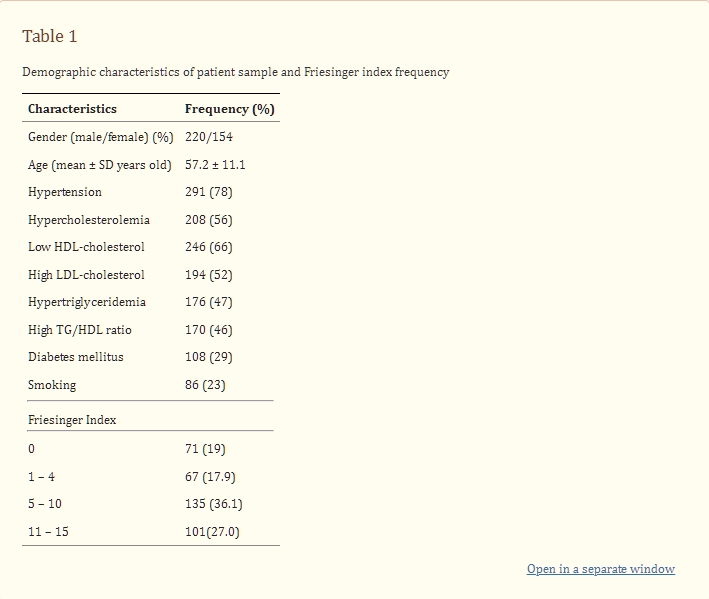
本研究納入了374名患者,其中165名(60.2%)男性和109名(39.8%)女性,平均年齡為57 ± 11.5歲。總膽固醇為214 ± 50.2 mg/dL;三酸甘油酯為167.9±91.7 mg/dL;HDL-c為38.5 ± 11.9 mg/dL;LDL-c為142.9 ± 45 mg/dL;TG/HDL-c為5.1 ± 4.0;Friesinger指數為6.9 ± 4.4。高血壓和脂質異常的受試者主要是男性。表1顯示了受試者樣本的人口統計信息,以及冠狀病變的分佈情況。
表1患者樣本的人口統計特徵和Friesinger指數頻率
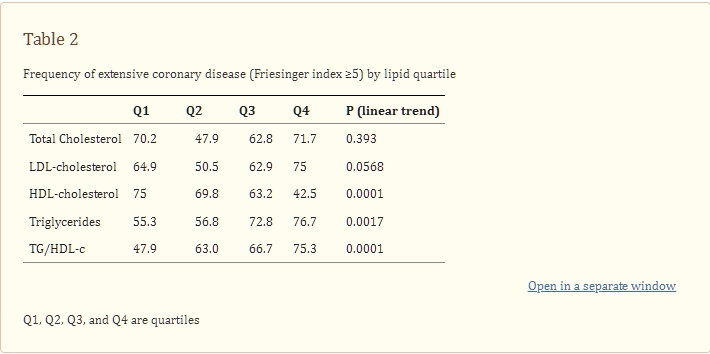
根據單變量分析,廣泛性冠心病與總三酸甘油酯四分位數和TG/HDL-c呈正相關,與HDL-c四分位數呈負相關(表2)。
表2冠狀動脈病變程度高(Friesinger指數≥5)的脂質四分位數頻率
冠狀動脈病變程度在第四和第一四分位數之間的勝算比如下:總膽固醇,1.08,95%CI(0.57–2.03),p = 0.87;LDL-c,1.62,95%CI(0.86–3.06),p = 0.15;三酸甘油酯,1.7,95%CI(0.94–3.08),p = 0.986;HDL-c,0.25,95%CI(0.13–0.46),p = 0.0001;以及TG/HDL-c,3.31,95%CI(1.78–6.14),p = 0.0002(圖1)。這個分析顯示,只有HDL-c和TG/HDL-c在第四和第一四分位數之間顯示出統計學上的頻率差異,而且對於TG/HDL-c的差異更大。非參數性ANOVA(Kruskal-Wallis)顯示了廣泛性冠心病和脂質變數四分位數之間的顯著關聯。然而,只有HDL-c和TG/HDL-c,主要是後者,顯示出異常值和正常值之間Friesinger指數的中位數在統計學上存在顯著差異。總膽固醇和LDL-c呈相似分佈,因此圖2只呈現了總膽固醇、三酸甘油酯、HDL-c和TG/HDL-c四分位數的Friesinger指數分佈。
圖1{kind=link}
脂質變數的第四和第一四分位數對於廣泛性冠心病(Friesinger指數> 4)的勝算比
圖2{kind=link}
根據總膽固醇、三酸甘油酯、高密度脂蛋白膽固醇和TG/HDL-膽固醇四分位數的Friesinger指數盒狀圖分佈
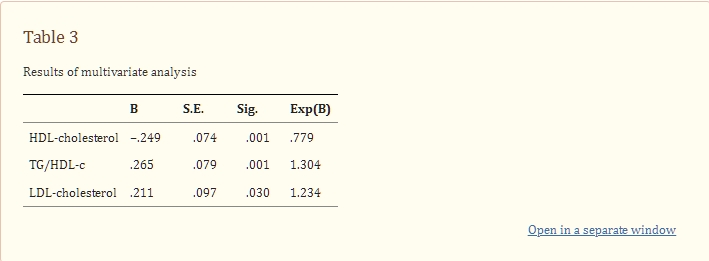
進行的多變量邏輯回歸分析包括這些脂質變數,並顯示TG/HDL-c比值與冠狀病變程度之間存在最強的相關性。提高HDL-c四分位數導致程度減少22%,而提高LDL-c或TG/HDL-c四分位數則分別導致疾病程度增加23%和30%(表3)。
表3多變量分析結果
在246名HDL-c水平低的受試者中,有171名(69.5%)患有廣泛性冠心病,而在170名TG/HDL-c高的受試者中,有122名(72%)患有廣泛性冠心病。這可能是因為HDL-c和三酸甘油酯水平在疾病程度較低的35名(25%)受試者和疾病程度較高的75名(32%)受試者中不一致。因此,通過使用三酸甘油酯到HDL-c比值考慮這兩個變數,提高了檢測廣泛性冠心病的準確性。
ROC曲線分析顯示以下曲線下面積:HDL-c為0.35(p = 0.0001),LDL-c為0.55(p = 0.131),TG/HDL-c為0.63(p = 0.0001)。
討論
我們通過單變量分析發現了冠狀病變程度與脂質變數之間的關係。在包括這些變數的多變量模型中,三酸甘油酯到高密度脂蛋白膽固醇比值被發現是廣泛性冠心病的有力獨立指標。
儘管小而密度高的LDL粒子是心血管疾病的確定危險因素,但通過當前方法評估其亞分別在例行臨床實驗室中應用技術過於要求。通常的技術包括密度梯度超速離心法、非變性梯度凝膠電泳(NDGGE)和核磁共振(NMR)光譜學,這些方法的缺點是勞動密集、技術要求高、昂貴或產生結果速度較慢。因此,這些精確和準確的技術在臨床環境中並不廣泛使用。因此,開發脂質粒子概況的替代標記對於臨床和經濟上至關重要。
幾項研究已試圖使用脂質指數或公式來確定冠狀動脈疾病的風險水平。10 這項工作的目標是更好地管理患者以預防心臟事件。特別感興趣的是分子中具有動脈粥樣硬化粒子的比值,分母中是高密度脂蛋白膽固醇或其組成部分。總膽固醇到HDL-c的比值,以及較小程度的LDL-c到HDL-c的比值已經被證明比單獨的脂質更好地預測了冠狀動脈疾病。最近,在INTERHEART病例對照研究中,apoB/apoA1比值被證明是與心肌梗塞相關的最強風險因素。該比值已經在AFCAPS/TexCAPS和AMORIS研究中被提議作為主要冠狀事件風險的準確預測因子。+
最初由Gaziano等人提出的TG/HDL-c比值是一個動脈粥樣硬化指數,已被證明是心肌梗塞的高度顯著獨立預測因子,甚至比TC/HDL-c和LDL-c/HDL-c更強。哥本哈根男性研究顯示,三酸甘油酯本身也是另一個強烈的風險因素,但它發現通過HDL-c水平對三酸甘油酯水平進行分層可以更準確地檢測冠心疾病風險的增加。
高三酸甘油酯和HDL-c之間的動脈粥樣硬化聯繫是由於三酸甘油酯富含的非常低密度脂蛋白在脂質交換和脂解過程中生成小而密度高的LDL。這些LDL粒子在循環中積累,形成小而密度高的HDL粒子,這些粒子經歷加速的分解代謝,因此封閉了動脈粥樣硬化循環。
本研究表明,我們之前已經顯示與冠心病發展相關的TG/HDL-c比值,也與血管受損的嚴重程度有關。因此,這個比值是一種簡單、非侵入性的方法,可以預測冠狀動脈粥樣硬化的存在和程度。
研究限制
我們研究了一個高風險的患者子集,其冠心病患病率高於一般人群。我們僅比較了脂質變數,未考慮患者目前使用的藥物或炎症狀態。由於常用的他汀類藥物、抑制蛋白酶和II型抑制劑可能改變炎症狀態,它們可能削弱了總膽固醇和LDL-膽固醇與冠心病程度之間的關係。這是因為它們對LDL-膽固醇的作用較多,對HDL-膽固醇和三酸甘油酯的作用較少。
結論
幾乎所有常規評估的脂質變數都與冠心病變程度相關,但只有三酸甘油酯到高密度脂蛋白膽固醇或到HDL-c的比值與疾病程度密切相關。 TG到HDL-c的比值的升高是所有檢查的脂質變數中對廣泛性冠心病的單一最強預測因子。
參考文獻
1. Miller NE. Associations of high-density lipoprotein subclasses and apolipoproteins with ischemic heart disease and coronary atherosclerosis. Am Heart J. 1987;113:589–97. [PubMed] [Google Scholar]
2. Robinson D, Ferns GA, Bevan EA, Stocks J, Williams PT, Galton DJ. High density lipoprotein subfractions and coronary risk factors in normal men. Arteriosclerosis. 1987;7:341–6. [PubMed] [Google Scholar]
3. Williams PT, Krauss RM, Vranizan KM, Stefanick ML, Wood PDS, Lindgren FT. Associations of lipoproteins and apolipoproteins with gradient gel electrophoresis estimates of high density lipoprotein subfractions in men and women. Arterioscler Thromb. 1992;12:332–40. [PubMed] [Google Scholar]
4. Hanak V, Munoz J, Teaque J, Stanley A, Jr, Bittner V. Accuracy of the triglyceride to high-density lipoprotein cholesterol ratio for prediction of the low-density lipoprotein phenotype B. Am J Cardiol. 2004;94:219–22. [PubMed] [Google Scholar]
5. Da luz PL, Cesena FH, Favarato D, Cerqueira ES. Comparison of serum lipid values in patients with coronary artery disease at <50, 50 to 59, 60 to 69, and >70 years of age. Am J Cardiol. 2005;96:1640–3. [PubMed] [Google Scholar]
6. Rinqqvist I, Fisher LD, Mock M, Davis KB, Wedel H, Chaitman BR, et al. The Coronary Artery Surgery Study. Prognostic Value of Angiographic Indices of Coronary Artery Disease from the Coronary Artery Surgery Study (CASS) J Clin Invest. 1983;71:1854–66. [PMC free article] [PubMed] [Google Scholar]
7. Krauss RM, Burke DJ. Identification of multiple subclasses of plasma low density lipoprotein in normal humans. J Lipid Res. 1982;23:97–104. [PubMed] [Google Scholar]
8. Scheffer PG, Bakker SJL, Heine RJ, Teerlink T. Measurement of LDL particle size in whole plasma and serum by high performance gel-filtration chromatography using a fluorescent lipid probe. Clin Chem. 1998;44:2148–51. [PubMed] [Google Scholar]
9. Kuller L, Arnold A, Tracy R, Otvos J, Burke G, Psaty B, et al. Nuclear Magnetic Resonance Spectroscopy of Lipoproteins and Risk of Coronary Heart Disease in the Cardiovascular Health Study. Arterioscler Thromb Vasc Biol. 2002;22:1175–80. [PubMed] [Google Scholar]10. Ballantyne CM, Hoogeveen RC. Role of lipid and lipotrotein profiles in risk assessment and therapy. Am Heart J. 2003;146:227–33. [PubMed] [Google Scholar]11. Hong MK, Romm PA, Reagan K, Green CE, Rackley CE. Usefulness of the total cholesterol to high density lipoprotein cholesterol ratio in predicting angiographic coronary disease in women. Am J Cardiol. 1991;68:1646–50. [PubMed] [Google Scholar]
12. Castelli WP, Anderson K, Wilson PW, Levy D. Lipids and risk of coronary heart disease. The Framingham Study. Ann Epidemiol. 1992;2:23–8. [PubMed] [Google Scholar]
13. Manninen V, Tenkanen L, Koshinen P, Huttunen JK, Manttari M, Heinonen PO, et al. Join effects of serum triglycerides and LDL cholesterol and HDL cholesterol concentrations on coronary heart disease risk in the Helsinki Heart Sudy. Implications for treatment. Circulation. 1992;85:37–45. [PubMed] [Google Scholar]
14. Yusuf S, Hawken S, Ounpuu S, Dans T, Avezum A, Lanas F, et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet. 2004;363:937–52. [PubMed] [Google Scholar]
15. Gotto AM, Jr, Whitney E, Stein EA, Shapiro DR, Clearfield, Weis S, et al. Relation between baseline and on-treatment lipid parameters and first acute major coronary event in the Air Force/Texas Coronary Atherosclerosis Prevention Study (AFCAPS/Tex CAPS) Circulation. 2000;101:477–84. [PubMed] [Google Scholar]
16. Walldius G, Jungner I, Holme I, Astveit AH, Kolar W, Steiner E. High apoliprotein B, low apolipoprotein A-I, and improvement in the prediction of fatal myocardial infarction (AMORIS Study): a prospective study. Lancet. 2001;358:2026–33. [PubMed] [Google Scholar]
17. Gaziano JM, Hennekens CH, O’Donnell CJ, Breslow JL, Buring JE. Fasting triglycerides, high density lipoprotein, and risk of myocardial infarction. Circulation. 1997;96:2520–5. [PubMed] [Google Scholar]
18. Jeppesen J, Hein HO, Suadicani P, Gyntelberg F. Triglycerides concentration and ischemic heart disease: an eight-year follow-up in the Copenhagen Male Study. Circulation. 1998;97:1029–36. [PubMed] [Google Scholar]
19. Packard CJ, Shepherd J. Lipoprotein heterogenity and apolipoprotein B metabolism. Arterioscler Thromb Vasc Biol. 1999;19:2456–64. [PubMed] [Google Scholar]
20. Brinton EA, Eeisenberg S, Breslow JL. Increased apo A-I and apo-AII fractional catabolic rate in patients with low high density lipoprotein-cholesterol levels with or without hypertriglyceridemia. J Clin Invest. 1991;87:536–44. [PMC free article] [PubMed] [Google Scholar]