

 English
English Bahasa Melayu
Bahasa Melayu Bahasa Indonesia
Bahasa Indonesia Tiếng Việt
Tiếng Việt ไทย
ไทย
本翻譯僅作學術交流用,無商業意圖,請勿轉載,如有疑議問請來信
一項大規模的網絡和配對元分析研究270項隨機對照試驗,涉及15,827名參與者,發現有氧運動、動態阻力訓練、結合訓練、高強度間歇訓練及等張運動訓練均顯著降低靜息收縮壓和舒張壓。其中,等張運動訓練對降低收縮壓和舒張壓最為有效。此研究為預防和治療動脈高血壓提供了全面的數據驅動框架。
運動訓練與靜息血壓:一項大規模成對和網絡薈萃分析的隨機對照試驗
Exercise training and resting blood pressure: a large-scale pairwise and network meta-analysis of randomised controlled trials
Edwards JJ, Deenmamode AHP, Griffiths M, et alExercise training and resting blood pressure: a large-scale pairwise and network meta-analysis of randomised controlled trialsBritish Journal of Sports Medicine 2023;57:1317-1326.
https://bjsm.bmj.com/content/57/20/1317
Abstract
Objective
To perform a large-scale pairwise and network meta-analysis on the effects of all relevant exercise training modes on resting blood pressure to establish optimal antihypertensive exercise prescription practices.
Design
Systematic review and network meta-analysis.
Data sources
PubMed (Medline), the Cochrane library and Web of Science were systematically searched.
Eligibility criteria
Randomised controlled trials published between 1990 and February 2023. All relevant work reporting reductions in systolic blood pressure (SBP) and/or diastolic blood pressure (DBP) following an exercise intervention of ≥2 weeks, with an eligible non-intervention control group, were included.
Results
270 randomised controlled trials were ultimately included in the final analysis, with a pooled sample size of 15 827 participants. Pairwise analyses demonstrated significant reductions in resting SBP and DBP following aerobic exercise training (−4.49/–2.53 mm Hg, p<0.001), dynamic resistance training (–4.55/–3.04 mm Hg, p<0.001), combined training (–6.04/–2.54 mm Hg, p<0.001), high-intensity interval training (–4.08/–2.50 mm Hg, p<0.001) and isometric exercise training (–8.24/–4.00 mm Hg, p<0.001). As shown in the network meta-analysis, the rank order of effectiveness based on the surface under the cumulative ranking curve (SUCRA) values for SBP were isometric exercise training (SUCRA: 98.3%), combined training (75.7%), dynamic resistance training (46.1%), aerobic exercise training (40.5%) and high-intensity interval training (39.4%). Secondary network meta-analyses revealed isometric wall squat and running as the most effective submodes for reducing SBP (90.4%) and DBP (91.3%), respectively.
Conclusion
Various exercise training modes improve resting blood pressure, particularly isometric exercise. The results of this analysis should inform future exercise guideline recommendations for the prevention and treatment of arterial hypertension.
摘要
目的
進行一項大規模的成對和網絡薈萃分析,探討所有相關運動訓練方式對靜息血壓的影響,以確立最佳的降血壓運動處方實踐。
設計
系統評論和網絡薈萃分析。
數據來源
系統搜索了PubMed(Medline)、Cochrane圖書館和Web of Science。
資格標準
1990年至2023年2月間發表的隨機對照試驗。納入了所有報告運動干預≥2週後收縮壓(SBP)和/或舒張壓(DBP)降低的相關工作,且有合適的非干預對照組。
結果
最終分析中包括了270項隨機對照試驗,共有15,827名參與者。成對分析顯示,有氧運動訓練(-4.49/-2.53毫米汞柱,p<0.001)、動態阻力訓練(-4.55/-3.04毫米汞柱,p<0.001)、結合訓練(-6.04/-2.54毫米汞柱,p<0.001)、高強度間歇訓練(-4.08/-2.50毫米汞柱,p<0.001)和等長運動訓練(-8.24/-4.00毫米汞柱,p<0.001)均顯著降低靜息SBP和DBP。網絡薈萃分析顯示,基於累積排序曲線下面積(SUCRA)值對SBP的有效性排名順序分別是等長運動訓練(SUCRA: 98.3%)、結合訓練(75.7%)、動態阻力訓練(46.1%)、有氧運動訓練(40.5%)和高強度間歇訓練(39.4%)。次級網絡薈萃分析顯示,等長壁蹲和跑步是分別降低SBP(90.4%)和DBP(91.3%)最有效的子方式。
結論
各種運動訓練方式可改善靜息血壓,尤其是等長運動。這項分析的結果應該為未來關於動脈高血壓預防和治療的運動指南推薦提供信息。
引言
高血壓是導致疾病和死亡的主要可修改風險因素。1-3 雖然在指南中對診斷切點的差異存在,4 5 但高於最佳水平的血壓與心血管疾病風險的直線相關聯。6 隨著高血壓的發病率增加,7 特別是在中低收入國家,8 對有效的降血壓干預的研究仍然至關重要。藥物療法是降低血壓的有效手段9;然而,不良的依從性,10-12 不良副作用13 和經濟支出14 是重要的限制。因此,非藥物方法受到青睞。15 16 運動明確地產生心血管健康益處並改善長期存活率,體力活動與減少死亡率的縱向關聯已被充分記錄。17-20
以前的大規模分析報告了來自不同運動方式的顯著收縮壓和舒張壓(SBP和DBP)降低。21-26 基於以前的工作,傳統的有氧運動訓練(AET)仍是管理靜息血壓的主要推薦運動方法。4 5 然而,當前的運動指南建議主要基於較舊的數據,而近期的調查顯示了對更新穎運動方式的日益興趣,如高強度間歇訓練(HIIT)27 和等長運動訓練(IET),24 以及對獨立的動態阻力訓練(RT)28 和結合RT和AET的新數據的大量研究。29 30 因此,管理靜息血壓的最佳運動干預是未知的,現有指南可能已經過時。
因此,這項工作旨在提供一項更新的大規模系統評論和隨機對照試驗(RCTs)的網絡薈萃分析(NMA),研究運動訓練對靜息SBP和DBP的影響。我們旨在對每種運動方式進行獨立的成對薈萃分析,隨後進行比較性的貝葉斯NMA。我們還旨在進行單獨的基線血壓分層分析,以確定每種運動方式對不同血壓分類人群的影響。
方法學
搜索策略
本次評論按照系統評論和薈萃分析的首選報告項目(PRISMA)指南執行,31 32 並在PROSPERO註冊(CRD42022326565)。為了確定報告運動訓練干預對靜息血壓影響的隨機對照試驗(RCTs),制定了一項全面的電子數據庫搜索策略。系統搜索是在PubMed(Medline)、Cochrane圖書館和Web of Science中進行的,使用了包括運動、體力活動、血壓和高血壓等相關醫學主題標題(MeSH)術語和文本詞的組合,並配合布林搜索詞“OR”和“AND”(在線補充附件A)。沒有使用搜索過濾器或限制。此外,單獨檢索了先前系統評論和薈萃分析的參考文獻列表,以查找在初始搜索中未確定的額外報告。考慮1990年至2023年2月期間發表的試驗為合適。
篩選和研究資格
在系統搜索之後,兩位作者(AD和OA)獨立篩選所有論文的合格性。研究最初通過標題和摘要進行篩選,如果符合預定的納入標準,則隨後通過全文進行篩選。研究人員討論了任何不一致和分歧,並在必要時與第四位研究人員(JE)達成共識。在研究招募之後,通過Microsoft Excel提取了所有納入研究的相關數據。第三位審稿人(MG)獨立評估和驗證了所有數據提取。最初提取了基線和干預後的收縮壓(SBP)和舒張壓(DBP)均值(SD)數據,因為運動訓練和血壓RCTs中通常沒有報告變化數據。為了進行NMA,我們獲得了基線和干預後值的平均變化。根據《Cochrane系統評論干預手冊》(第6章),33 我們目標是從標準誤差、95% CI、p值或t統計數據計算SD變化。當研究沒有報告任何此類數據時,SD變化是使用之前在類似數據集中測試和驗證的相關係數0.8計算的。22
根據參與者、干預、比較對象、結果(PICO)框架,人口包括成年人,沒有對健康或疾病狀態的預定限制,代表一般人口,這確保我們不會不必要地排除任何可能有價值的數據。考慮到這項工作的干預、比較對象和結果,如果試驗被適當隨機化,並在運動和非干預對照組中報告了干預前和後的SBP和/或DBP,則確定為合格。為了最小化混淆,非干預對照組中任何顯著的飲食、諮詢或運動影響導致排除。同樣,包含與運動同時進行的共同干預(如補充或藥物變化)的研究被排除。僅考慮同行評審期刊上發表的試驗,因此不符合資格的論文論文。對於可能看起來符合條件但被排除的研究,可以向相應的作者(並附上排除的原因)請求。
為了保持一致性,每篇納入的論文的運動協議/強度都根據日常實踐和康復訓練中的運動處方(EXPERT)工具34 進行篩選並進行定義和分類。然後,所有協議被分類為以下主要運動方式類別之一:“有氧運動訓練”(AET)、“動態阻力訓練”(RT)、“結合訓練”(CT)、“高強度間歇訓練”(HIIT)和“等長運動訓練”(IET)。然後進一步探索每個類別的適當亞組,允許分析步行、跑步和自行車作為AET亞組,衝刺間歇訓練(SIT)和有氧間歇訓練(AIT)作為HIIT亞組,以及等長握力(IHG)、等長腿部伸展(ILE)和等長壁蹲(IWS)作為IET亞組。IET程序通常使用4×2分鐘收縮的協議,中間有1-4分鐘的休息間隔,每週進行三次。IHG通常處方為最大自願收縮的30%,而IWS和ILE協議通常在實驗室基礎最大等長運動測試期間達到的峰值心率的95%下進行。IWS也可以使用自選壁蹲處方,膝關節角度會引起第一回合感知努力率(RPE)為3.5-4.5/10;第二回合RPE為5-6/10;第三回合RPE為6.5-7.5/10;第四回合RPE為8-9/10。這篇評論將HIIT定義為“短暫高強度運動的間歇性爆發,由低強度恢復期隔開”。35 作為HIIT的亞組,SIT被定義為“全力以赴”的最大低體積協議,而有氧間歇訓練AIT由4×4分鐘的較低強度協議組成。
對於基線血壓分層分析,所有納入的研究根據干預組和對照組的基線SBP和DBP被分類為正常血壓、前期高血壓或高血壓。根據歐洲高血壓學會/歐洲心臟學會(ESC/ESH)指南,5 SBP和DBP狀態亞組被分類為正常血壓、前期高血壓或高血壓,值分別為<130/85毫米汞柱,130-139/85-89毫米汞柱或>140/90毫米汞柱。在這項分析中,干預組和對照組在基線血壓類別上不同的研究被排除。
研究質量
偏見風險和方法學嚴謹性使用TESTEX量表進行評估。36 TESTEX是一個15分(12項)工具,專為評估運動訓練試驗而設計。如先前在這類大規模評論中所示,22從每種運動方式中隨機選取了10%的試驗進行偏見風險評估。兩位審稿人(AD和JE)獨立對所有選定的文章進行評分。質量分析中的任何爭議都通過共識解決。
統計分析
成對薈萃分析使用Comprehensive Meta-Analysis,版本3(Biostat,Englewood,New Jersey,USA)進行。分別對每個主要(AET,RT,CT,HIIT,IET)和次要(步行,騎自行車,跑步,SIT,AIT,IHG,IWS和ILE)運動方式組進行合並分析,以確定運動組與非干預對照組在SBP和DBP的加權平均差異(WMD)。在沒有任何心血管或其他疾病的研究中也進行了平行的合並分析。然後,根據基線血壓分類進一步將每個主要運動方式組分為兩類並分別進行分析。進行了薈萃回歸分析,以確定是否有任何研究級調節變量影響血壓變化並解釋觀察到的結果間研究的變異。獨立運行的選定調節器是干預持續時間(以週計)、訓練頻率(每週次數)和訓練依從性(參加規定課程的平均百分比)。統計異質性始終與合並分析一起測試並報告為I²統計。對I²統計應用40%的顯著性閾值。37 一旦超過此閾值,像Egger’s迴歸測試(1997)這樣的事後測試就會系統地計劃來評估漏斗圖不對稱性以解釋潛在的出版偏見。38 固定或隨機效應方法的選擇取決於異質性的存在,當通過顯著異質性確認了研究間的變異時,應用隨機效應分析。合並分析的結果在p值<0.05並且Z值>2時被認為是顯著的。
為了促進尚未在RCT中直接比較的運動方式的比較,並通過包括直接和間接數據來提高比較效果估計的精確度,我們進行了NMA。貝葉斯NMA通過MetaInsight工具(版本V4.0.2)進行。39 MetaInsight是一個由Rshiny提供動力的互動式網絡工具,它使用R軟件包「gemtc」和「BUGSnet」進行貝葉斯統計計算。該分析運行Markov鏈蒙特卡洛模擬,共有四個鏈和總共25,000次迭代(燒錄期5000)。通過Gelman-Rubin收斂評估測試模型的收斂。40 基於預先確立的研究間異質性,選擇隨機效應分析WMD。通過節點分裂模型評估直接和間接效果大小比較的不一致性41,並給出相應的貝葉斯P值。為了NMA產生了具有一致性模型和無關平均效果不一致模型的殘差偏差圖。對於任何具有較大殘差偏差(>2)的研究,進一步探索並計劃在敏感性分析中排除。為了評估基線SBP和DBP的調節效果,分別使用WinBUGS版本1.4.42進行了貝葉斯NMA薈萃回歸分析。
分別對主要運動方式分類(AET,RT,CT,HIIT和IET)和次要運動亞組分類(步行,跑步,騎自行車,RT,CT,SIT,AIT,IHG,ILE,IWS)進行了單獨的NMA。由於沒有為RT和CT預先確立次要運動方式分類,因此它們被包括在兩種分析中。製作了網絡圖以可視化不同運動方式之間的直接和間接比較。NMA數據報告為平均效果及其95%可信區間。進行了排名概率分析,為每種運動方式和亞組生成了累積排名曲線下面積(SUCRA)值,並顯示為試紙排名圖SUCRA圖。43
圖1 PRISMA系統評論和薈萃分析流程圖。RCT,隨機對照試驗。{kind=link}
結果
圖1顯示了PRISMA系統評論流程圖。初始系統搜索識別出14,553項試驗,通過篩選先前的薈萃分析及其各自的參考文獻列表,發現了額外的138項試驗。經過所有排除後,最終納入了270項運動訓練隨機對照試驗(RCTs),涵蓋了15,827名(其中7,632名對照組)參與者的分析樣本。分析涉及358個效應大小,包括182個AET(89步行,28騎自行車,21跑步和44「其他」AET),57個RT,46個CT,49個HIIT(其中7個為SIT和13個為AIT)和24個IET(17個IHG,4個IWS,3個ILE)。完整的TESTEX偏見風險評估得分可以在線補充表S1中找到。TESTEX評估顯示運動訓練文獻中存在幾個一貫的限制。特別是,大多數試驗未監測對照組活動或在適當時進行意向治療分析。所有270項試驗的研究和訓練特性在線補充表S2中呈現。為了敏感性和比較目的,我們還進行了平行的主要分析,排除了所有疾病(如2型糖尿病)。重要的是,這類疾病的納入/排除並不會顯著影響整體結果,相反,通常在排除有用數據後生成更寬的可信區間(見線上補充表S4)。每項分析的異質性結果可以在相應的圖形中找到。針對主要結果使用Comprehensive Meta-Analysis內置的「移除一項研究」分析方法進行了敏感性分析,這並未顯著影響任何總體效應大小。
成對分析
圖2顯示了與對照組相比,每種運動方式後的整體收縮壓(SBP)減少情況。所有類型的AET均顯著降低了SBP,整體降低了4.49毫米汞柱(95% CI 3.5到5.5,Z=8.8,prandom<0.001),步行降低了2.85毫米汞柱,騎自行車降低了6.88毫米汞柱,跑步降低了6.83毫米汞柱。事後Egger’s測試對AET整體SBP出版偏見顯著(線上補充圖S1)。RT降低了4.55毫米汞柱的SBP(95% CI 3.2到5.9,Z=6.6,prandom<0.001),CT降低了6.04毫米汞柱(95% CI 3.2到8.9,Z=4.1,prandom<0.001)。儘管HIIT整體降低了4.08毫米汞柱的SBP(95% CI 2.6到5.5,Z=5.5,prandom<0.001)且SIT降低了5.26毫米汞柱,但AIT並未顯著變化。所有IET模式都顯著降低了SBP,整體降低了8.24毫米汞柱(95% CI 6.5到10.0,Z=9.0,prandom<0.001),IHG降低了7.10毫米汞柱,ILE降低了10.05毫米汞柱,IWS降低了10.47毫米汞柱。
圖2 森林圖展示了每種主要和次要運動方式對收縮壓(SBP)的整體影響。{kind=link}
圖3森林圖展示了與對照組相比,每種運動方式後的整體舒張壓(DBP)減少情況。所有類型的AET均顯著降低了DBP,整體降低了2.53毫米汞柱(95% CI 1.8到3.2,Z=7.3,prandom<0.001),步行降低了1.44毫米汞柱,騎自行車降低了3.20毫米汞柱,跑步降低了5.67毫米汞柱。事後Egger’s測試對AET整體DBP出版偏見顯著(線上補充圖S2)。RT降低了3.04毫米汞柱的DBP(95% CI 2.2到3.9,Z=6.9,prandom<0.001),CT降低了2.54毫米汞柱(95% CI 1.1到4.0,Z=3.4,prandom=0.001)。儘管HIIT整體降低了2.50毫米汞柱的DBP(95% CI 1.2到3.8,Z=3.8,prandom<0.001)且SIT降低了3.29毫米汞柱(95% CI 0.1到6.5,Z=2.0,prandom=0.043),但AIT並未顯著變化。所有IET模式都顯著降低了DBP,整體降低了4.0(95% CI 2.7到5.3,Z=6.0,prandom<0.001),IHG降低了3.46毫米汞柱,ILE降低了4.23毫米汞柱,IWS降低了5.33毫米汞柱。事後Egger’s測試對IET整體DBP出版偏見顯著(線上補充圖S3)。
圖3 森林圖展示了每種主要和次要運動方式對舒張壓(DBP)的整體影響。{kind=link}
圖4展示了根據基線血壓狀態分層的每種運動方式的收縮壓(SBP)減少情況。除了CT和HIIT的前期高血壓組分析外,所有分析都統計顯著。雖然所有運動方式在正常血壓群體中均顯示出統計上顯著的SBP減少,但在高血壓患者中所有減少幅度顯著更大。由於數據有限,舒張壓(DBP)的此類基線類別分層分析無法進行。
第4圖 森林圖描述了每種主要運動方式對收縮壓(SBP)在基線血壓分類下的總體影響。{kind=link}
正如在網上補充表格S3中所示,有氧運動訓練(AET)的收縮壓(SBP)調節變數交互作用是顯著的,較低的訓練頻率與更大的降壓效應相關(B=−1.0596,p=0.019)。對於其他任何運動方式,干預持續時間、訓練頻率或訓練依從性均無顯著的調節效應。
網絡元分析
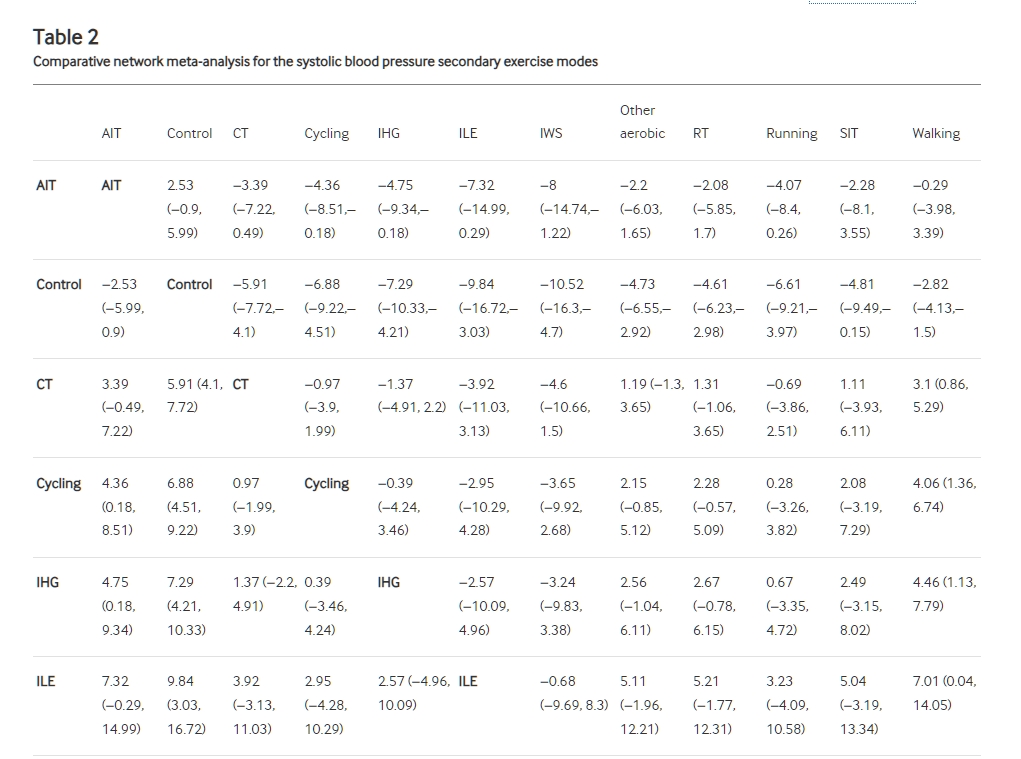
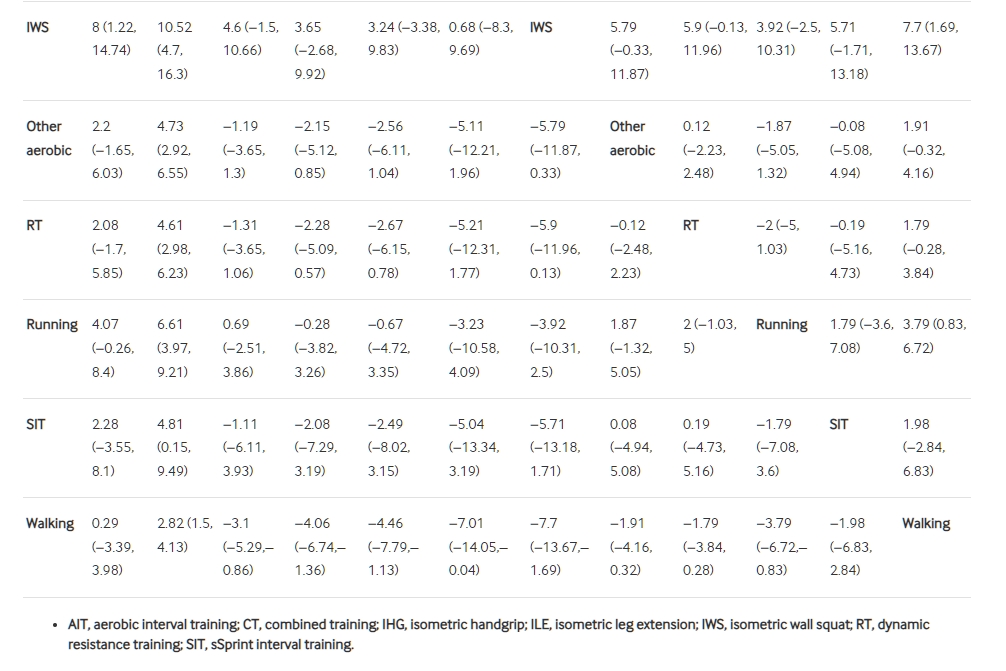
圖5顯示了帶有相應貝葉斯排名面板圖的網絡圖,而表1和表2,線上附加表S9和S10則詳細介紹了主要和次要運動SBP和DBP模式分析的比較NMA結果。高級分析結果,包括具有SUCRA的排名概率表(線上附加表S5、S6、S11和S12)、使用節點分裂模型進行不一致性測試(線上附加表S7、S8、S13和S14)以及偏差報告圖(線上附加圖S4、S5、S8和S9)可以在附加文件中找到。在主要或次要NMA中沒有不一致性的證據。
圖5{kind=link}
網絡圖示出主要和次要網絡元分析的直接和間接比較,以及相應的貝葉斯排名面板圖。AET,有氧運動訓練;AIT,有氧間歇訓練;CT,綜合訓練;HIIT,高強度間歇訓練;IET,等長運動訓練;IHG,等長手握;ILE,等長腿部伸展;IWS,等長壁壘深蹲;NMA,網絡元分析;RT,動態阻力訓練;SBP,收縮壓;SIT,短程間歇訓練;SUCRA,累積排名曲線下面積。
表1 主要運動模式的收縮壓比較網絡元分析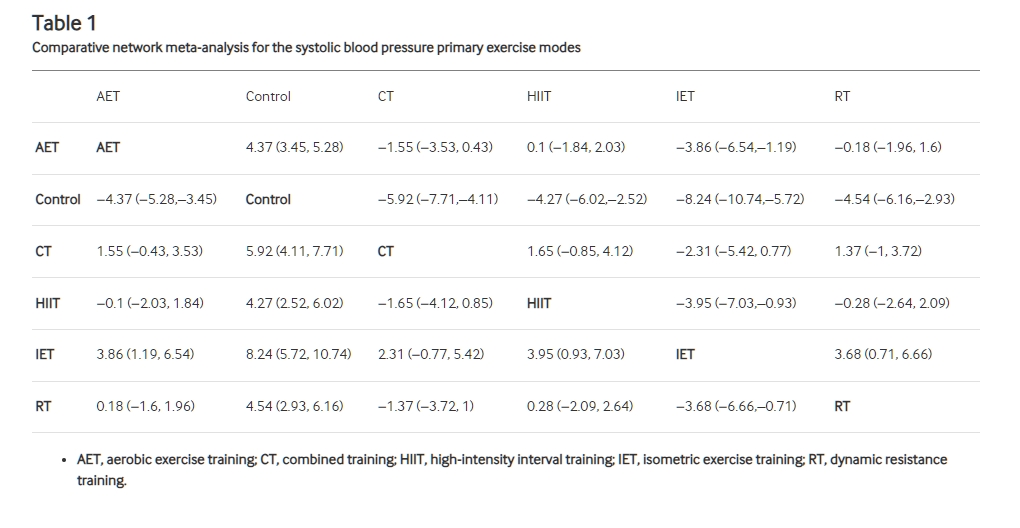
主要運動模式的SBP NMA包括305個兩臂研究,24個多臂試驗和11個直接比較。如表1和貝葉斯治療排名(圖5和表S5)所示,基於SUCRA值的有效性順序是IET(SUCRA:98.3%),CT(75.7%),RT(46.1%),AET(40.53%)和HIIT(39.44%)。相對而言,IET在降低SBP方面明顯比AET(WMD:-3.86 mm Hg,95% CI 1.19到6.54),HIIT(WMD:-3.95 mm Hg,95% CI 0.93到7.03)和RT(WMD:-3.68 mm Hg,95% CI 0.71到6.66)更有效。主要運動模式在SBP方面沒有其他顯著差異。與成對比較分析一致,NMA元回歸顯示基線SBP對各種運動模式有重要的調節作用。具體而言,平均基線對照組SBP增加1個單位,將使干預變化增加0.10 mm Hg(95% CI 0.05至0.15)。敏感性分析排除了總共3個殘差偏差>2的試驗(圖S10)。 CT的效應大小在敏感性分析中降低,因此在貝葉斯排名中降低了其位置,與主要分析相比,CT的效應大小提高了,而HIIT降低了。
次要運動模式SBP NMA包括282個兩臂研究,21個多臂試驗和21個直接比較。基於SUCRA值的有效性順序為IET IWS(90.4%),ILE(84.7%),IHG(73.1%),騎自行車(69.9%),跑步(66.1%),CT(57.6%),SIT(43.3%),其他有氧(40.1%),RT(38.2%),AIT(18.3%)和步行(17.4%)。相對而言,IWS、ILE、IHG、CT、騎自行車和跑步都明顯比步行更有效。 IWS、IHG和騎自行車也明顯比AIT更有效。次要運動模式在SBP方面沒有其他顯著差異。
主要運動模式的DBP NMA包括296個兩臂研究,24個多臂試驗和11個直接比較。基於SUCRA值的有效性順序(圖S6)是IET(89.0%),RT(67.6%),HIIT(51.5%),CT(46.7%)和AET(45.1%)。相對而言,主要運動模式在DBP方面沒有統計學上顯著的差異。與成對比較分析一致,NMA元回歸顯示基線DBP對各種運動模式有重要的調節作用。具體而言,平均基線對照組DBP增加1個單位,將使干預變化增加0.06 mm Hg(95% CI 0.01至0.12)。敏感性分析排除了總共5個殘差偏差>2的試驗(圖S11)。 CT的效應大小在敏感性分析中改善,而HIIT則在敏感性分析中降低,因此與主要分析相比,CT的位置增加,而HIIT的位置降低。
次要運動模式的DBP NMA包括274個兩臂研究,21個多臂試驗和21個直接比較。基於SUCRA值(圖S7)的有效性順序是跑步(91.3%),IWS(86.1%),IHG(57.1%),ILE(56.2%),騎自行車(54.3%),SIT(54.2%),RT(52.1%),AIT(48.1%),其他有氧(46.9%),CT(38.0%)和步行(14.7%)。相對而言,跑步、IWS、IHG、騎自行車和其他有氧比步行明顯更有效。跑步也明顯比CT、騎自行車、其他有氧和RT更有效。次要運動模式在DBP方面沒有其他顯著差異。
討論
在這個系統性回顧和NMA中,我們分析了所有相關的隨機對照試驗數據,涉及270個試驗和15,827名參與者,以建立在管理靜息動脈血壓方面的最佳運動處方實踐(見圖6)。成對比較分析顯示,除AIT外,所有運動模式均顯著降低了靜息SBP和DBP。所有模式均在高血壓患者中顯示出比正常基線血壓更大的降低。正如主要NMA所示,基於SUCRA值的SBP有效性排名順序是IET排名最高,其次是CT,RT,AET和HIIT。在DBP NMA中,IET也排名最高,其次是RT,HIIT,CT和AET。對於SBP的次要運動子模式的NMA發現IWS是最有效的,其次是ILE,IHG,騎自行車,跑步,CT,SIT,其他有氧,RT,AIT,最後是步行。DBP的次要NMA發現跑步是最有效的子模式,其次是IWS,IHG,ILE,騎自行車,SIT,RT,AIT,其他有氧,CT和步行。
圖6 中央圖示。AET,有氧運動訓練;CT,綜合訓練;HIIT,高強度間歇訓練;IET,等長運動訓練;RT,動態阻力訓練。{kind=link}
根據我們的知識,以前只有兩個類似比例的大規模荟萃分析研究曾經進行過。然而,本研究是首次將高強度間歇訓練(HIIT)納入為一種新型運動模式,並提供了有關步行、騎自行車、跑步、SIT、AIT、IHG、ILE和IWS的先進子模式分析,以優化運動處方。Cornelissen等人21也報告了等長運動訓練(IET)是最有效的運動模式,但在所有其他模式分析的幅度方面存在很大差異,這可能歸因於本研究中包含了大量新的試驗。這得到了更近期的Naci等人22 NMA的支持,該研究未評估DBP,但顯示AET、RT和CT的SBP變化較為一致,而不同於本研究。由於歐洲心臟病學會/歐洲高血壓學會(ESC/ESH)和美國心臟學院/美國心臟協會(ACC/AHA)的血壓管理指南都強調Cornelissen和Smart21研究的重要性,本研究的發現以及Naci等人22的研究結果表明需要更新運動建議指南。
Hanssen等人44的先前荟萃分析試圖通過間接比較不同運動模式的荟萃分析數據,來確定高血壓預防和治療中的最佳個性化運動處方實踐。與此不同,我們的工作採用了一種更直接的方法,通過統計比較所有單個RCTs來進行比較。因此,我們的研究結果存在差異,特別是對於IET,這部分可能歸因於Hanssen等人44必然依賴於舊的荟萃分析數據來總結IET當前有效性的事實,以及間接荟萃分析比較的內在限制。特別是,這個以前的總結分析顯示AET和RT的荟萃分析研究過多,與IET、CT和HIIT的荟萃分析工作過少,導致依賴於能力不足和過時的系統評論和荟萃分析數據來得出比較性結論。由於我們的分析直接從每個RCT中獲取了數據,因此在我們的工作中不存在RCT數據的傳播和最終轉化為已發表的荟萃分析研究之間的限制差距。
重要的是,這個更新的分析現在提供了大規模的數據,確立了CT作為一種有效的降低血壓的運動模式,以前被認為是由於證據不足而無法得出結論。Naci等人22以前報導了類似的SBP變化,但缺乏支持的DBP數據,而Hanssen等人44也對CT提供了支持,但只能根據單個荟萃分析做出有限的比較推論。盡管從CT中觀察到的降壓似乎與IET的降壓相當可比,但我們的新分析顯示,這種程度的CT降壓主要受到分析中包括的高血壓人群更多的影響。事實上,在正常血壓和高血壓前期人群的研究中,變化的幅度令人失望,NMA SBP敏感性分析顯示了這些數據集的脆弱性。相反,與以前的報告相反,RT現在似乎與AET在降低靜息血壓方面相當。然而,應注意的是,AET的有效性似乎取決於所進行的子模式,其中騎自行車和跑步明顯優於步行AET。我們的荟萃分析回歸分析還報告了在AET中,每週訓練頻率較低的情況下,SBP降低幅度較大。考慮到研究協議之間的差異,這一發現的原因尚不清楚,但可能提供了將AET應用於較低頻率(例如,每週3次)而不是大量每週(≥每週5次)的支持。
作為一種新的干預措施,高強度間歇訓練(HIIT)在SBP和DBP方面都產生了臨床相關的降低,但在所有主要模式中排名最低,SBP方面效果最差。次要子模式分析(成對和NMA)顯示,主要的SBP降低主要是由SIT(低容量,最大強度間隔)主導的,而AIT(4×4分鐘間隔)對於SBP或DBP都未達到統計學顯著水平。這一發現,再加上步行相對於跑步和騎自行車AET的比較差,似乎突顯了需要更高強度的訓練來產生最大的降低血壓效果。
與IET一樣,HIIT最近引起了廣泛的研究興趣,由於其節省時間且方便的特點,可能有增加採納和遵守的潛力,兩種模式都具有有前景的未來臨床效用。然而,本分析的結果支持我們以前的工作,認為IET是卓越的抗高血壓運動模式。雖然IET可能仍需要更大規模的長期RCT,其在管理正常、高血壓前期和高血壓個體的血壓方面的主要推薦運動模式的臨床應用得到了本研究的支持。重要的是,Cornelissen和Smart21的先前研究在2013年僅包括了四個IET試驗。自那時以來,在過去的十年中已發表了許多IET試驗和隨後的荟萃分析研究,本研究包括了19個RCT。因此,這一發現的置信區間已經大幅縮小,提供了更準確的SBP和DBP效應大小,分別為8.2和4.0mm Hg,與標準劑量的抗高血壓單藥療法相當。
限制
本研究存在一些限制需要認識。儘管本分析僅包括了隨機對照試驗(RCTs),但我們的TESTEX偏倚風險評估顯示,與運動訓練文獻一致,存在一些限制,包括對控制組活動監測不足、缺少意圖治療分析,以及參與者和研究者對組分配的認識。此外,由於進行了如此大規模的分析,我們不可避免地包括了不同參與者人群、統計和方法過程以及運動干預細節的試驗。作為這種試驗間變異性的一個可能結果,我們發現了大多數分析中存在顯著的異質性。此外,我們還發現了總體AET SBP和DBP以及IET DBP存在顯著的出版偏見。一些較新的運動模式,如SIT、AIT、ILE和IWS,涉及的RCTs較少,比較不像AET和RT等更成熟的模式。因此,這些子模式無法根據基線血壓狀態進行分層和分析。最後,本分析中包括的大多數RCTs在其分析中設定了先前的最低出席閾值(例如,完成>80%的課程)。因此,我們的培訓遵從性調節分析預設情況下不包括低出勤率,這些結果應僅在評估已經遵守的個體中的遵守調節效應的背景下解釋。
結論
有氧運動訓練、動態阻力訓練、綜合訓練、高強度間歇訓練和等長運動訓練在降低靜息SBP和DBP方面都具有顯著的有效性。相比之下,等長運動訓練仍然是最有效的模式。本分析的結果應該為未來的指南建議提供信息。
參考文獻
↵ Lim SS , Vos T , Flaxman AD , et al . A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012;380:2224–60. doi:10.1016/S0140-6736(12)61766-8 CrossRefPubMedWeb of ScienceGoogle Scholar
↵ Murray CJL , Aravkin AY , Zheng P , et al . Global burden of 87 risk factors in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020;396:1223–49. doi:10.1016/S0140-6736(20)30752-2 CrossRefPubMedGoogle Scholar
↵ Yusuf S , Joseph P , Rangarajan S , et al . Modifiable risk factors, cardiovascular disease, and mortality in 155 722 individuals from 21 high-income, middle-income, and low-income countries (PURE): a prospective cohort study. Lancet 2020;395:795–808. doi:10.1016/S0140-6736(19)32008-2 CrossRefPubMedGoogle Scholar
↵ Whelton PK , Carey RM , Aronow WS , et al . ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: executive summary: A report of the American college of cardiology/American heart Association task F. J Am Soc Hypertens 2018;12:S1933-1711(18)30189-X. doi:10.1016/j.jash.2018.06.010 Google Scholar
↵ Williams B , Mancia G , Spiering W , et al . ESC/ESH guidelines for the management of arterial hypertension. Eur Heart J 2018;39:3021–104. doi:10.1093/eurheartj/ehy339 CrossRefPubMedGoogle Scholar
↵ Bundy JD , Li C , Stuchlik P , et al . Systolic blood pressure reduction and risk of cardiovascular disease and mortality a systematic review and network meta-analysis. JAMA Cardiol 2017;2:775–81. doi:10.1001/jamacardio.2017.1421 Google Scholar
↵ Mills KT , Stefanescu A , He J . The global epidemiology of hypertension. Nat Rev Nephrol 2020;16:223–37. doi:10.1038/s41581-019-0244-2 PubMedGoogle Scholar
↵ Zhou B , Carrillo-Larco RM , Danaei G , et al . Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: a pooled analysis of 1201 population-representative studies with 104 million participants. Lancet 2021;398:957–80. doi:10.1016/S0140-6736(21)01330-1 PubMedGoogle Scholar
↵ Rahimi K , Bidel Z , Nazarzadeh M , et al . Pharmacological blood pressure lowering for primary and secondary prevention of cardiovascular disease across different levels of blood pressure: an individual participant-level data meta-analysis. Lancet 2021;397:1625–36. doi:10.1016/S0140-6736(21)00590-0 CrossRefPubMedGoogle Scholar
↵ Vrijens B , Vincze G , Kristanto P , et al . Adherence to prescribed antihypertensive drug treatments: longitudinal study of electronically compiled dosing histories. BMJ 2008;336:1114–7. doi:10.1136/bmj.39553.670231.25 Abstract/FREE Full TextGoogle Scholar
↵ Choudhry NK , Kronish IM , Vongpatanasin W , et al . Medication adherence and blood pressure control: a scientific statement from the American Heart Association. Hypertension 2022;79:e1–14. doi:10.1161/HYP.0000000000000203 CrossRefPubMedGoogle Scholar
↵ Burnier M , Egan BM . Adherence in hypertension. Circ Res 2019;124:1124–40. doi:10.1161/CIRCRESAHA.118.313220 CrossRefPubMedGoogle Scholar
↵ Cohen JS . Adverse drug effects, compliance, and initial doses of antihypertensive drugs recommended by the joint national committee vs the physicians’ desk reference. Arch Intern Med 2001;161:880. doi:10.1001/archinte.161.6.880 Google Scholar
↵ Wang G , Grosse SD , Schooley MW . Conducting research on the economics of hypertension to improve cardiovascular health. Am J Prev Med 2017;53:S115–7. doi:10.1016/j.amepre.2017.08.005 CrossRefPubMedGoogle Scholar
↵ Cernota M , Kroeber ES , Demeke T , et al . Non-pharmacological interventions to achieve blood pressure control in African patients: a systematic review. BMJ Open 2022;12:e048079. doi:10.1136/bmjopen-2020-048079 Google Scholar
↵ Valenzuela PL , Carrera-Bastos P , Gálvez BG , et al . Lifestyle interventions for the prevention and treatment of hypertension. Nat Rev Cardiol 2021;18:251–75. doi:10.1038/s41569-020-00437-9 CrossRefGoogle Scholar
↵ Lear SA , Hu W , Rangarajan S , et al . The effect of physical activity on mortality and cardiovascular disease in 130 000 people from 17 high-income, middle-income, and low-income countries: the PURE study. Lancet 2017;390:2643–54. doi:10.1016/S0140-6736(17)31634-3 CrossRefPubMedGoogle Scholar
↵ Leitzmann MF , Park Y , Blair A , et al . Physical activity recommendations and decreased risk of mortality. Arch Intern Med 2007;167:2453–60. doi:10.1001/archinte.167.22.2453 CrossRefPubMedWeb of ScienceGoogle Scholar
↵ Wang Y , Nie J , Ferrari G , et al . Association of physical activity intensity with mortality: a national cohort study of 403 681 US adults. JAMA Intern Med 2021;181:203–11. doi:10.1001/jamainternmed.2020.6331 Google Scholar
↵ Blond K , Brinkløv CF , Ried-Larsen M , et al . Association of high amounts of physical activity with mortality risk: a systematic review and meta-analysis. Br J Sports Med 2020;54:1195–201. doi:10.1136/bjsports-2018-100393 Abstract/FREE Full TextGoogle Scholar
↵ Cornelissen VA , Smart NA . Exercise training for blood pressure: a systematic review and meta-analysis. J Am Heart Assoc 2013;2:e004473. doi:10.1161/JAHA.112.004473 Google Scholar
↵ Naci H , Salcher-Konrad M , Dias S , et al . How does exercise treatment compare with antihypertensive medications? A network meta-analysis of 391 randomised controlled trials assessing exercise and medication effects on systolic blood pressure. Br J Sports Med 2019;53:859–69. doi:10.1136/bjsports-2018-099921 Abstract/FREE Full TextGoogle Scholar
↵ Whelton SP , Chin A , Xin X , et al . Effect of aerobic exercise on blood pressure: a meta-analysis of randomized, controlled trials. Ann Intern Med 2002;136:493–503. doi:10.7326/0003-4819-136-7-200204020-00006 CrossRefPubMedWeb of ScienceGoogle Scholar
↵ Edwards J , De Caux A , Donaldson J , et al . Isometric exercise versus high-intensity interval training for the management of blood pressure: a systematic review and meta-analysis. Br J Sports Med 2022;56:506–14. doi:10.1136/bjsports-2021-104642 Abstract/FREE Full TextGoogle Scholar
↵ Cornelissen VA , Fagard RH , Coeckelberghs E , et al . Impact of resistance training on blood pressure and other cardiovascular risk factors. Hypertension 2011;58:950–8. doi:10.1161/HYPERTENSIONAHA.111.177071 CrossRefPubMedGoogle Scholar
↵ Lee L-L , Mulvaney CA , Wong YKY , et al . Walking for hypertension. Cochrane Database Syst Rev 2021;2:CD008823. doi:10.1002/14651858.CD008823.pub2 Google Scholar
↵ Costa EC , Hay JL , Kehler DS , et al . Effects of high-intensity interval training versus moderate-intensity continuous training on blood pressure in adults with pre- to established hypertension: a systematic review and meta-analysis of randomized trials. Sports Med 2018;48:2127–42. doi:10.1007/s40279-018-0944-y CrossRefPubMedGoogle Scholar
↵ Ashton RE , Tew GA , Aning JJ , et al . Effects of short-term, medium-term and long-term resistance exercise training on cardiometabolic health outcomes in adults: systematic review with meta-analysis. Br J Sports Med 2020;54:341–8. doi:10.1136/bjsports-2017-098970 Abstract/FREE Full TextGoogle Scholar
↵ Xi H , He Y , Niu Y , et al . Effect of combined aerobic and resistance exercise on blood pressure in postmenopausal women: a systematic review and meta-analysis of randomized controlled trials. Exp Gerontol 2021;155:S0531-5565(21)00342-9. doi:10.1016/j.exger.2021.111560 Google Scholar
↵ Schroeder EC , Franke WD , Sharp RL , et al . Comparative effectiveness of aerobic, resistance, and combined training on cardiovascular disease risk factors: a randomized controlled trial. PLoS One 2019;14:e0210292. doi:10.1371/journal.pone.0210292 Google Scholar
↵ Page MJ , McKenzie JE , Bossuyt PM , et al . The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. doi:10.1136/bmj.n71 Google Scholar
↵ Hutton B , Salanti G , Caldwell DM , et al . The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann Intern Med 2015;162:777–84. doi:10.7326/M14-2385 Available: https://doi.org/107326/M14-2385 CrossRefPubMedGoogle Scholar
↵ Higgins JPT , Li T , Deeks JJ . Choosing effect measures and computing estimates of effect. Cochrane Handbook for Systematic Reviews of Interventions 2019:143–76. doi:10.1002/9781119536604 Google Scholar
↵ Hansen D , Dendale P , Coninx K , et al . The European Association of Preventive Cardiology Exercise Prescription in Everyday Practice and Rehabilitative Training (EXPERT) tool: a digital training and decision support system for optimized exercise prescription in cardiovascular disease. concept, definitions and construction methodology. Eur J Prev Cardiol 2017;24:1017–31. doi:10.1177/2047487317702042 CrossRefPubMedGoogle Scholar
↵ Campbell WW , Kraus WE , Powell KE , et al . High-intensity interval training for cardiometabolic disease prevention. Med Sci Sports Exerc 2019;51:1220–6. doi:10.1249/MSS.0000000000001934 CrossRefPubMedGoogle Scholar
↵ Smart NA , Waldron M , Ismail H , et al . Validation of a new tool for the assessment of study quality and reporting in exercise training studies: TESTEX. Int J Evid Based Healthc 2015;13:9–18. doi:10.1097/XEB.0000000000000020 CrossRefPubMedGoogle Scholar
↵ Huedo-Medina TB , Sánchez-Meca J , Marín-Martínez F , et al . Assessing heterogeneity in meta-analysis: Q Statistic or I 2 index Psychol Methods 2006;11:193–206. doi:10.1037/1082-989X.11.2.193 CrossRefPubMedWeb of ScienceGoogle Scholar
↵ Egger M , Smith GD , Schneider M , et al . Bias in meta-analysis detected by a simple, graphical test. BMJ 1997;315:629–34. doi:10.1136/bmj.315.7109.629 Abstract/FREE Full TextGoogle Scholar
↵ Owen RK , Bradbury N , Xin Y , et al . MetaInsight: an interactive web‐based tool for analyzing, interrogating, and visualizing network meta‐analyses using R‐Shiny and Netmeta. Res Synth Methods 2019;10:569–81. doi:10.1002/jrsm.1373 Google Scholar
↵ Brooks SP , Gelman A . n.d. General methods for monitoring convergence of Iterative simulations.Google Scholar
↵ Dias S , Welton NJ , Sutton AJ , et al . Evidence synthesis for decision making 4: inconsistency in networks of evidence based on randomized controlled trials. Med Decis Making 2013;33:641–56. doi:10.1177/0272989X12455847 CrossRefPubMedWeb of ScienceGoogle Scholar
↵ Lunn DJ , Thomas A , Best N , et al . WinBUGS – A Bayesian modelling framework: concepts, structure, and extensibility. Stat Comput 2000;10:325–37. doi:10.1023/A:1008929526011 CrossRefWeb of ScienceGoogle Scholar
↵ Nevill CR , Cooper NJ , Sutton AJ . A multifaceted graphical display, including treatment ranking, was developed to aid interpretation of network meta-analysis. J Clin Epidemiol 2023;157:83–91. doi:10.1016/j.jclinepi.2023.02.016 Google Scholar
↵ Hanssen H , Boardman H , Deiseroth A , et al . Personalized exercise prescription in the prevention and treatment of arterial hypertension: a consensus document from the European Association of Preventive Cardiology (EAPC) and the ESC Council on Hypertension. Eur J Prev Cardiol 2022;29:205–15. doi:10.1093/eurjpc/zwaa141 Google Scholar
↵ Carlson DJ , Dieberg G , Hess NC , et al . Isometric exercise training for blood pressure management: a systematic review and meta-analysis. Mayo Clin Proc 2014;89:327–34. doi:10.1016/j.mayocp.2013.10.030 CrossRefPubMedWeb of ScienceGoogle Scholar
↵ Kelley GA , Kelley KS . Isometric handgrip exercise and resting blood pressure: a meta-analysis of randomized controlled trials. J Hypertens 2010;28:411–8. doi:10.1097/HJH.0b013e3283357d16 CrossRefPubMedWeb of ScienceGoogle Scholar
↵ Corso LML , Macdonald HV , Johnson BT , et al . Is concurrent training efficacious antihypertensive therapy? A meta-analysis. Med Sci Sports Exerc 2016;48:2398–406. doi:10.1249/MSS.0000000000001056 CrossRefPubMedGoogle Scholar
↵ Goessler K , Polito M , Cornelissen VA . Effect of exercise training on the renin–angiotensin–aldosterone system in healthy individuals: a systematic review and meta-analysis. Hypertens Res 2016;39:119–26. doi:10.1038/hr.2015.100 Google Scholar
↵ Ekkekakis P , Biddle SJH . Extraordinary claims in the literature on high-intensity interval training (HIIT): IV. is HIIT associated with higher long-term exercise adherence Psychology of Sport and Exercise 2023;64:102295. doi:10.1016/j.psychsport.2022.102295 Google Scholar
↵ Batacan RB , Duncan MJ , Dalbo VJ , et al . Effects of high-intensity interval training on cardiometabolic health: a systematic review and meta-analysis of intervention studies. Br J Sports Med 2017;51:494–503. doi:10.1136/bjsports-2015-095841 Abstract/FREE Full TextGoogle Scholar
↵ Millar PJ , McGowan CL , Cornelissen VA , et al . Evidence for the role of Isometric exercise training in reducing blood pressure: potential mechanisms and future directions. Sports Med 2014;44:345–56. doi:10.1007/s40279-013-0118-x CrossRefPubMedGoogle Scholar
↵ Stensvold D , Viken H , Steinshamn SL , et al . Effect of exercise training for five years on all cause mortality in older adults—the generation 100 study: randomised controlled trial. BMJ 2020;371:m3485. doi:10.1136/bmj.m3485 Google Scholar
↵ Edwards JJ , Taylor KA , Cottam C , et al . Ambulatory blood pressure adaptations to high-intensity interval training: a randomized controlled study. J Hypertens 2021;39:341–8. doi:10.1097/HJH.0000000000002630 CrossRefPubMedGoogle Scholar
↵ MacInnis MJ , Gibala MJ . Physiological adaptations to interval training and the role of exercise intensity. J Physiol 2017;595:2915–30. doi:10.1113/JP273196 Available: http://doi.wiley.com/10.1113/tjp.2017.595.issue-9 CrossRefPubMedGoogle Scholar
↵ O’Driscoll JM , Edwards JJ , Coleman DA , et al . One year of Isometric exercise training for blood pressure management in men: a prospective randomized controlled study. J Hypertens 2022;40:2406–12. doi:10.1097/HJH.0000000000003269 Google Scholar
↵ Edwards JJ , Wiles J , O’Driscoll J . Mechanisms for blood pressure reduction following Isometric exercise training: a systematic review and meta-analysis. J Hypertens 2022;40:2299–306. doi:10.1097/HJH.0000000000003261 Google Scholar
↵ Inder JD , Carlson DJ , Dieberg G , et al . Isometric exercise training for blood pressure management: A systematic review and meta-analysis to optimize benefit. Hypertens Res 2016;39:88–94. doi:10.1038/hr.2015.111 CrossRefPubMedGoogle Scholar
↵ López-Valenciano A , Ruiz-Pérez I , Ayala F , et al . Updated systematic review and meta-analysis on the role of Isometric resistance training for resting blood pressure management in adults. J Hypertens 2019;37:1320–33. doi:10.1097/HJH.0000000000002022 CrossRefPubMedGoogle Scholar
↵ Sánchez-Meca J , Marín-Martínez F . Confidence intervals for the overall effect size in random-effects meta-analysis. Psychol Methods 2008;13:31–48. doi:10.1037/1082-989X.13.1.31 CrossRefPubMedWeb of ScienceGoogle Scholar
↵ Law MR , Morris JK , Wald NJ . Use of blood pressure lowering drugs in the prevention of cardiovascular disease: meta-analysis of 147 randomised trials in the context of expectations from prospective epidemiological studies. BMJ 2009;338:b1665. doi:10.1136/bmj.b1665 Google Scholar
↵ Paz MA , de-La-Sierra A , Sáez M , et al . Treatment efficacy of anti-hypertensive drugs in monotherapy or combination: ATOM systematic review and meta-analysis of randomized clinical trials according to PRISMA statement. Medicine (Baltimore) 2016;95:e4071. doi:10.1097/MD.0000000000004071 Google Scholar
↵ Pagonas N , Vlatsas S , Bauer F , et al . Aerobic versus Isometric handgrip exercise in hypertension: a randomized controlled trial. J Hypertens 2017;35:2199–206. doi:10.1097/HJH.0000000000001445 Google Scholar
↵ Goessler KF , Buys R , VanderTrappen D , et al . A randomized controlled trial comparing home-based Isometric Handgrip exercise versus endurance training for blood pressure management. J Am Soc Hypertens 2018;12:285–93. doi:10.1016/j.jash.2018.01.007 Google Scholar